
Chapter 2: The 5 Movement Dysfunctions

Soft Tissue
When we discuss soft tissue we are commenting on organs, bones, muscle, tendon, and ligaments. Complete tears of muscle and ligament, and early tumors do not typically cause pain, because all the pain receptors have been disrupted.
Partial tears and organ pathology can cause pain. This pain will be specific, palpable and unchanging. Soft tissue dysfunction results in a true weakness that does not resolve when the mechanical joint dysfunction is treated. Fixing the mechanical joint dysfunction first allows you to see what symptoms remain so you can better understand the extent of the problem and can make an appropriate referral if necessary.
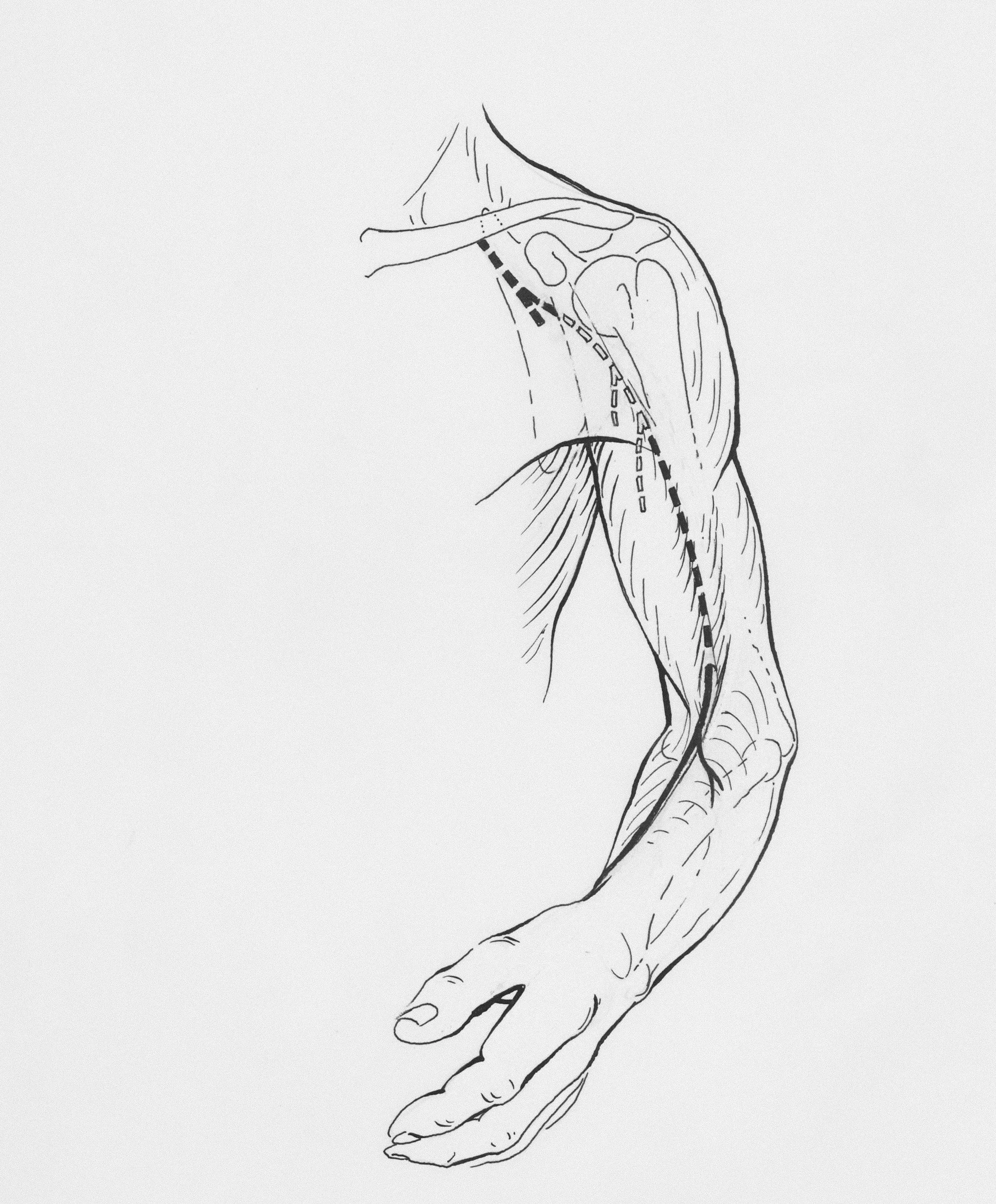
Peripheral Nerve
Neurological dysfunction will present with three specific signs: decreased reflexes, numbness and decreased strength without pain. If there are no neurological signs with radicular symptoms along a dermatome then the irritation is probably the somatic referred symptoms from the mechanical joint dysfunction.
For a quick neurological test in the event of back pain, have the patient walk on his toes and heels to test the possibility of nerve impingement at L4 and S1 respectively. The clinician needs to strength test to check the remaining levels as well. Movement can be painless or painful, weak or strong. A presentation of weakness and no pain means that there is a complete neurological rupture. This needs to be referred immediately to a neurosurgeon.
Reflexes will be decreased on the affected side if there is a neurological dysfunction, with a different reflex being affected for each nerve root. The biceps tendon reflex arc passes through the fifth and sixth segments of the cervical cord levels, along with the brachioradialis reflex arc. The triceps tendon reflex arc passes through the sixth, seventh and eight cord levels. The patellar tendon reflex arc passes through the second, third and the forth lumbar cord levels. And the Achilles reflex arc passes through the first, second and sacral cord levels.
Sensation will also decrease with a neurological dysfunction. This will present as a true numbness that defines a specific pattern down the limb. Overlapping areas of sensory nerve supply are common. However, there should be a definitive pattern of persistent sensory loss to suggest a neurological dysfunction.
Systemic Inflammatory Issue
Irritation due to an inflammatory processes presents symmetrically on the right and left sides of the body. When we suggest a systemic inflammatory process we are discussing a rheumatological phenomenon, an immune system deficiency.
Neurologically reflexes will be intact but can be hyper due to inflammation or to the nerve irritation and the associated pain. Swelling can be present, but remember that detecting swelling with palpation is only accurate twenty percent of the time. Movement will be painful and hesitant or strong. Activity level will decrease over time as pain and movement limitations persist. Morning irritation will be a pattern and will last more than thirty minutes. There will be complaints of stiffness upon moving after sitting or standing. Fixing the mechanics will decrease the irritation but will not resolve the entire presentation.
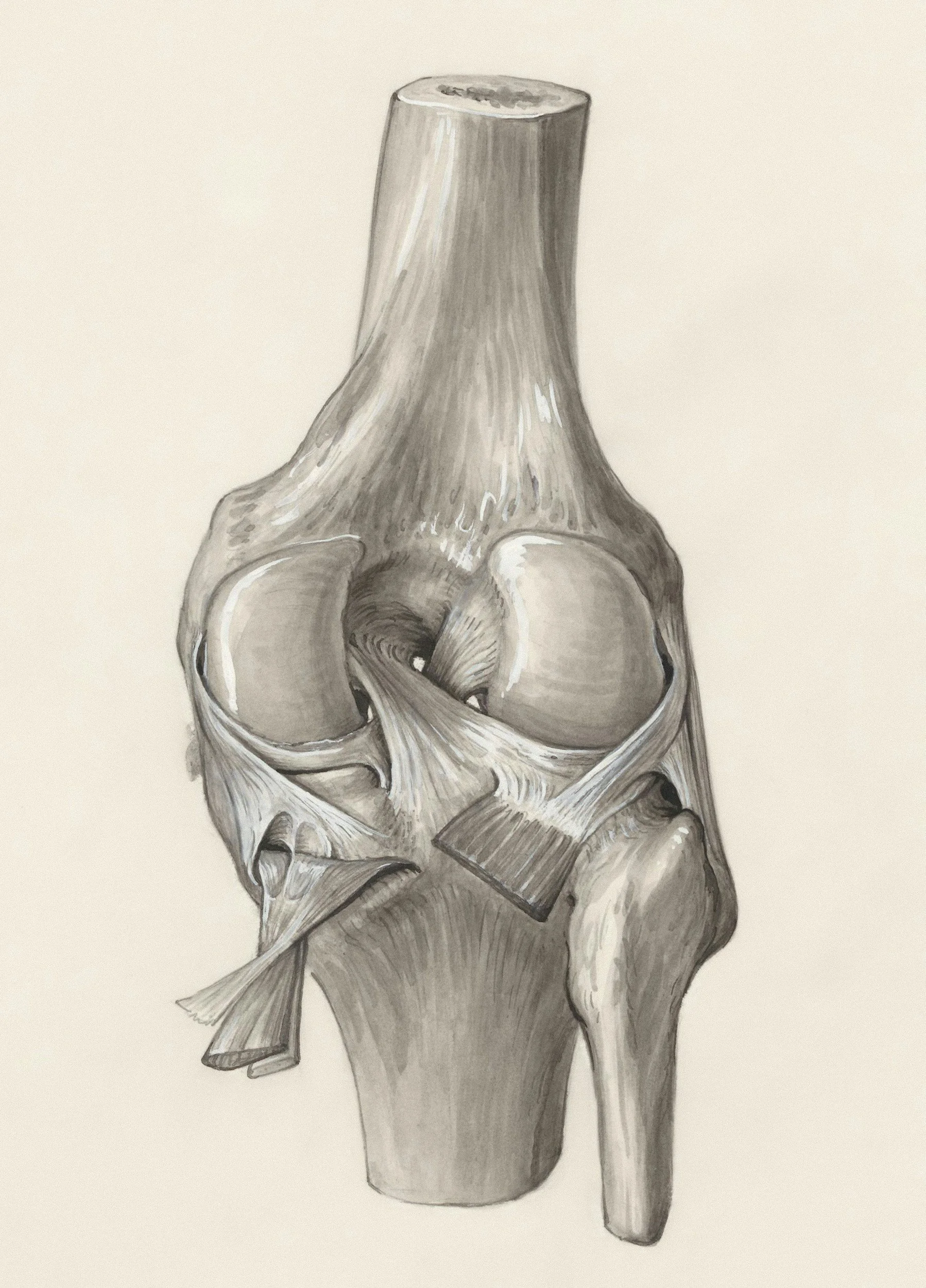
Osteoarthritic Change
In a healthy joint, the ends of the bones are covered in smooth, resilient cartilage. This cartilage acts as a cushion and allows the bones to glide against each other without friction. An osteoarthritic change occurs when this protective cartilage begins to break down.
The smooth cartilage surface becomes frayed, rough, and thinner over time. As the cartilage wears away, the bones can start to rub directly against each other. The tissues and lining of the joint can become inflamed, leading to swelling and pain. The underlying bone can become thicker and harder (sclerosis), and the ligaments and tendons that support the joint may weaken.
The most prevalent symptom, joint pain is often worse during or after activity and can be relieved by rest. In more advanced stages, the pain may be constant, even at rest. A feeling of joint stiffness, especially in the morning or after periods of inactivity (e.g., sitting for a long time). This stiffness usually eases within 30 minutes after you start moving.
The affected joint may not be able to move through its full range of motion. The joint may swell, which can be caused by fluid accumulation or the presence of bone spurs.
Mechanical Joint Dysfunction
Mechanical joint dysfunction appears as a decrease of movement accompanied by increased muscle tone, muscle tightness, and muscle inhibition.
Mechanical joint dysfunction is the inability of a joint to move in all available planes of movement within its preferred path, impairing function at the joint and limiting muscle performance. This impairment is associated with the sensation of pain and a secondary muscle spasm. Tissue entrapment of the joint capsule occurs with uncontrolled movement and results in the firing of nociceptors and ultimately the sensation of pain. The release of chemical irritants by associated tissue will increase the sensitivity to pain.
Mechanical dysfunction is the diagnosis, and pain associated with a spasm is the experience. A patient complaining of back pain also complains of loss of movement. Pain produced at the joint level puts the supporting muscles into spasm and prevents full joint play. The passive range of motion available at a joint depends on the shape of the articular surfaces as well as the pliability of the surrounding soft tissues. Active range of motion of the soft tissue is approximately equal to the accompanying joint’s passive range of motion. When passive and active movement at the joint is limited, mechanical dysfunction has occurred. Muscles cannot move a joint that is not free to move.